SRFP092: Sociodemographic Trends in the Location of Federally Qualified Health Center 340B Program Enrollment Before & After the ACA
Reshma Ramachandran, MD, MPP
Abstract
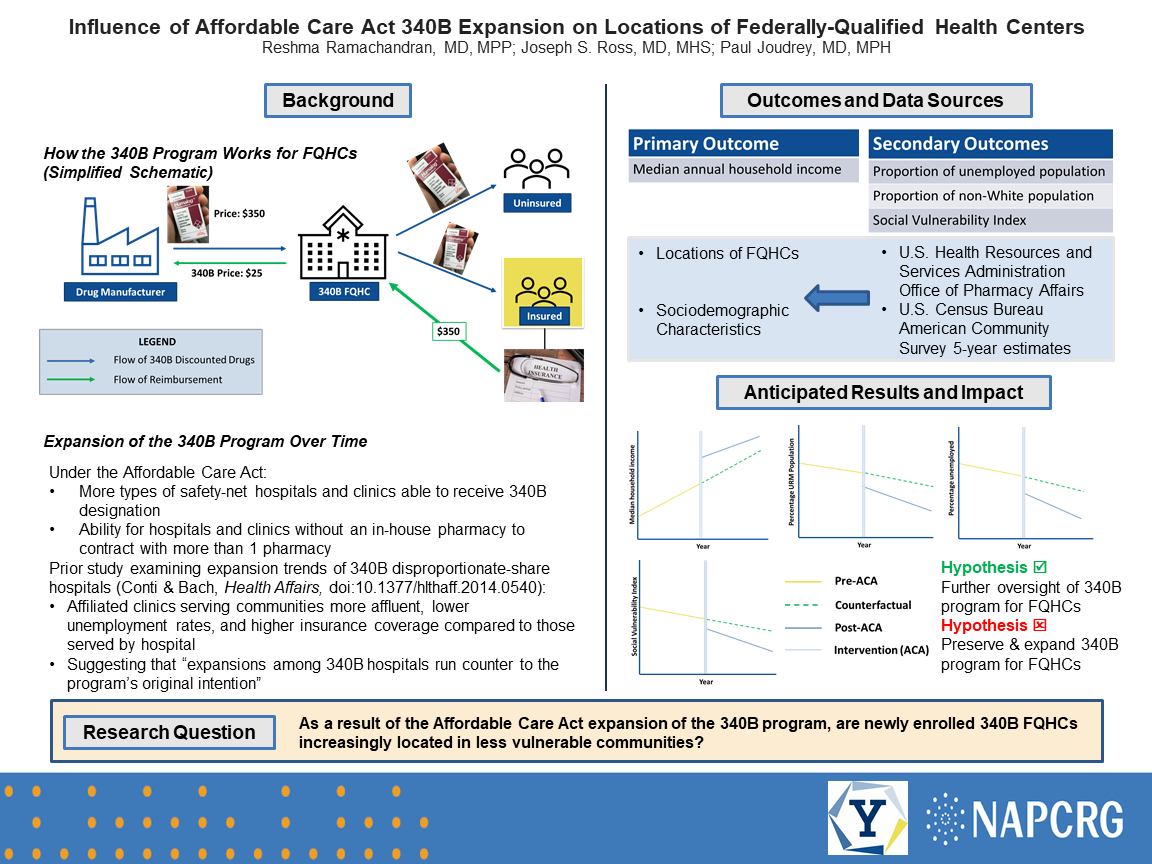
Context: Federally qualified health center (FQHCs) participation in the 340B program expanded under the 2010 Patient Protection and Affordable Care Act (ACA). Under the ACA, FQHCs without in-house pharmacies are now able to contract with outside pharmacies to provide 340B discounted drugs. The 340B program is intended to provide assistance to uninsured and low-income patients through significant discounts for outpatient medications. However, prior studies have demonstrated that newly enrolled 340B hospital-affiliated clinics were more likely to be in more affluent areas with higher rates of insurance coverage. It is unclear if a similar trend can be seen with FQHCs meant to provide primary care services to medically underserved and vulnerable populations. Objective: To determine whether the ACA 340B expansion helped narrow socioeconomic and racial disparities in the locations of newly enrolled FQHCs. Study Design/Dataset/Population Studied: Interrupted time series analysis of newly enrolled FQHC locations extracted from yearly Health Resources and Services Administration national 340B program data from 2005 to 2019, including those within the U.S. and its territories and excluding those that could not be located to a ZIP code tabulation area (ZCTA). ZCTA sociodemographic data will be obtained from the U.S. Census Bureau American Community Survey. Main and Secondary Outcome Measures: Main outcome - yearly ZCTA median income for newly enrolled 340B FQHCs. Secondary outcomes - yearly proportion of the ZCTA population that is non-Hispanic White for newly enrolled 340B FQHCs; yearly counts of all newly enrolled FQHCs among all ZCTAS and those within low-income and majority-minority ZCTAs. Anticipated Results: Newly enrolled 340B FQHCs will be located within wealthier ZCTAs and ZCTAS with higher proportions of non-Hispanic White residents after implementation of the ACA 340B changes. Yearly ZCTA median income and proportion non-Hispanic White of 340B FQHC locations will increase over time. Conclusions: Covered entities can purchase significantly discounted 340B drugs while charging private payers the traditional price thereby maximizing revenue by providing care for commercially insured patients. If the findings reflect anticipated results, this would suggest that ACA 340B changes are contributing to geographic inequities in new FQHC locations and could prompt further scrutiny of the program to better target patient populations intended for the 340B program.
Jack Westfall
jwestfall@aafp.org 11/21/2021Terrific project. Great poster and abstract. Thanks for sharing at NAPCRG