SRFP070: Mixed Methods Systematic Review of Physician use of Race in Medical Decision-making
Ebiere Okah, MD; LaShaunta Glover; Gaurav Dave; Katrina Donahue, MD, MPH; Giselle Corbie-Smith, MD, MSc
Abstract
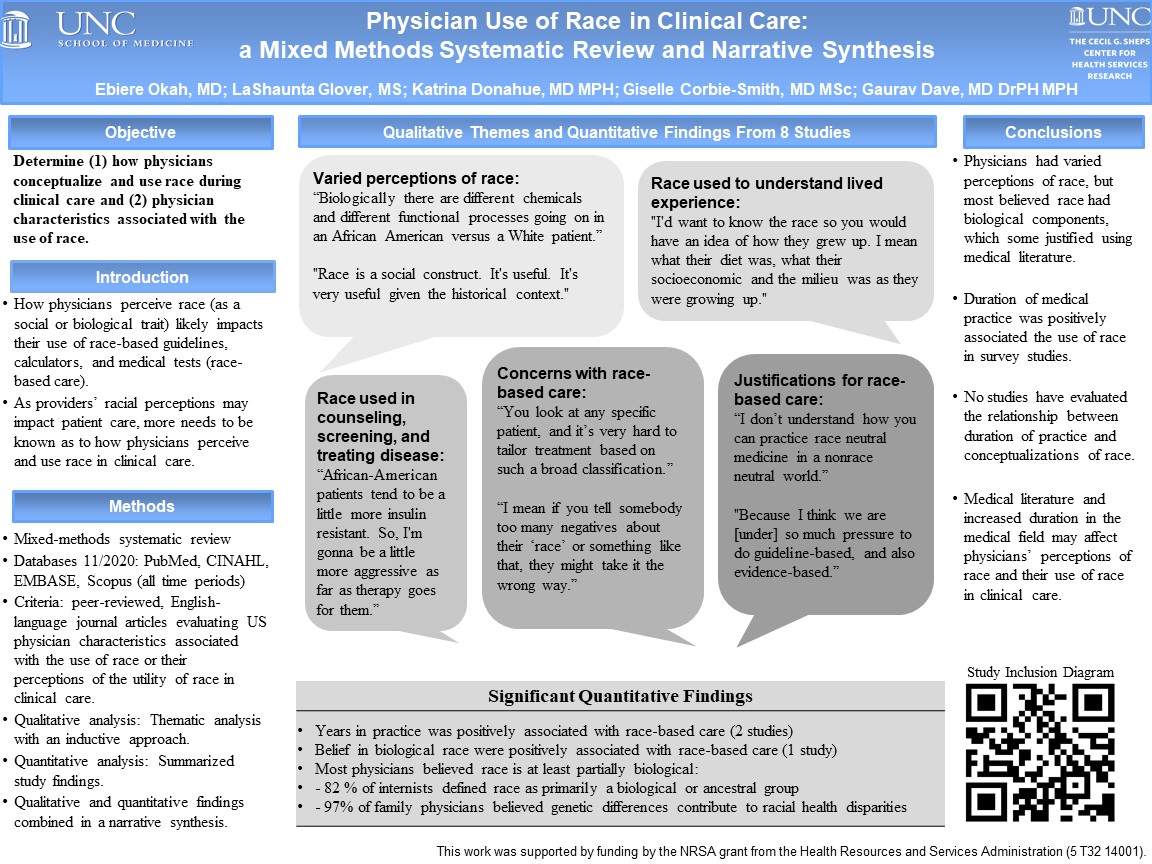
Context: Medical guidelines recommend that physicians use race to select antihypertensive medications and determine the risk of vaginal birth after cesarean. However, physicians conceptualize race in varied ways (i.e., social or biological construct) which may impact their use of race-based medical guidelines and calculators and, therefore, affect patient care. Objective: To determine (1) how physicians conceptualize and use race in their clinical care and (2) physician characteristics associated with the use of race. Study Design: This is a mixed-methods systematic review. Two independent reviewers completed the title and abstract review, full-text review, and quality assessment, with discrepancies resolved by consensus or a third reviewer. Data extraction was conducted collaboratively by two reviewers. Themes from qualitative studies were elicited using an inductive approach with thematic analysis. Qualitative and quantitative findings were combined using a narrative synthesis. Setting or Dataset: A comprehensive search (using iterations of the following terms: “race,” “clinical decision-making,” and “physicians”) of PubMed, CINAHL, EMBASE, and Scopus was conducted. Population studied: English-language, peer-reviewed journal articles based on research studies evaluating US physicians’ conceptualizations and use of race in clinical practice. Outcome measures: Physicians’ conceptualization and use of race in clinical care. Results: In total, 1,049 articles were identified; of these, eight studies (four qualitative and four quantitative) met the inclusion criteria. Preliminary findings indicate that most physicians believed race was clinically relevant and viewed the race as having biological components, using results from medical studies to justify this belief. Physicians used race to gain insight into their patient’s biopsychosocial factors (i.e., culture, behaviors, socioeconomic status, and genetic risk for disease). They used these “insights” to guide clinical care (i.e., counseling, testing, treatment). Some physicians voiced concerns about using race, citing unclear racial boundaries, provider discomfort, and patient mistrust of race-based care. Conclusions: Physicians view race as a trait that allows them to better understand their patient’s social context and genetic risk. Additional research is needed to determine the extent to which physicians use race as a substitute for individual patient characteristics.
Debora Goldberg
dgoldbe4@gmu.edu 11/20/2021Ebiere, LaShaunta, and others Great work that illustrates the need for continued research on structural racism in healthcare delivery. I cringed when I read some of those quotes, and realized how important it is to document these thoughts and viewpoints to better understand the problem and develop solutions for health equity. Through my own research I realized the importance of understanding individual patient preferences for care. Good luck on your future research. Debora