SRFP002: A Qualitative Analysis of Patient Perspectives on Low Value Healthcare and the Patient-Clinician Relationship
Kenan Michaels, BA; John Epling, MD, MSEd; Michelle Rockwell, PhD, RD
Abstract
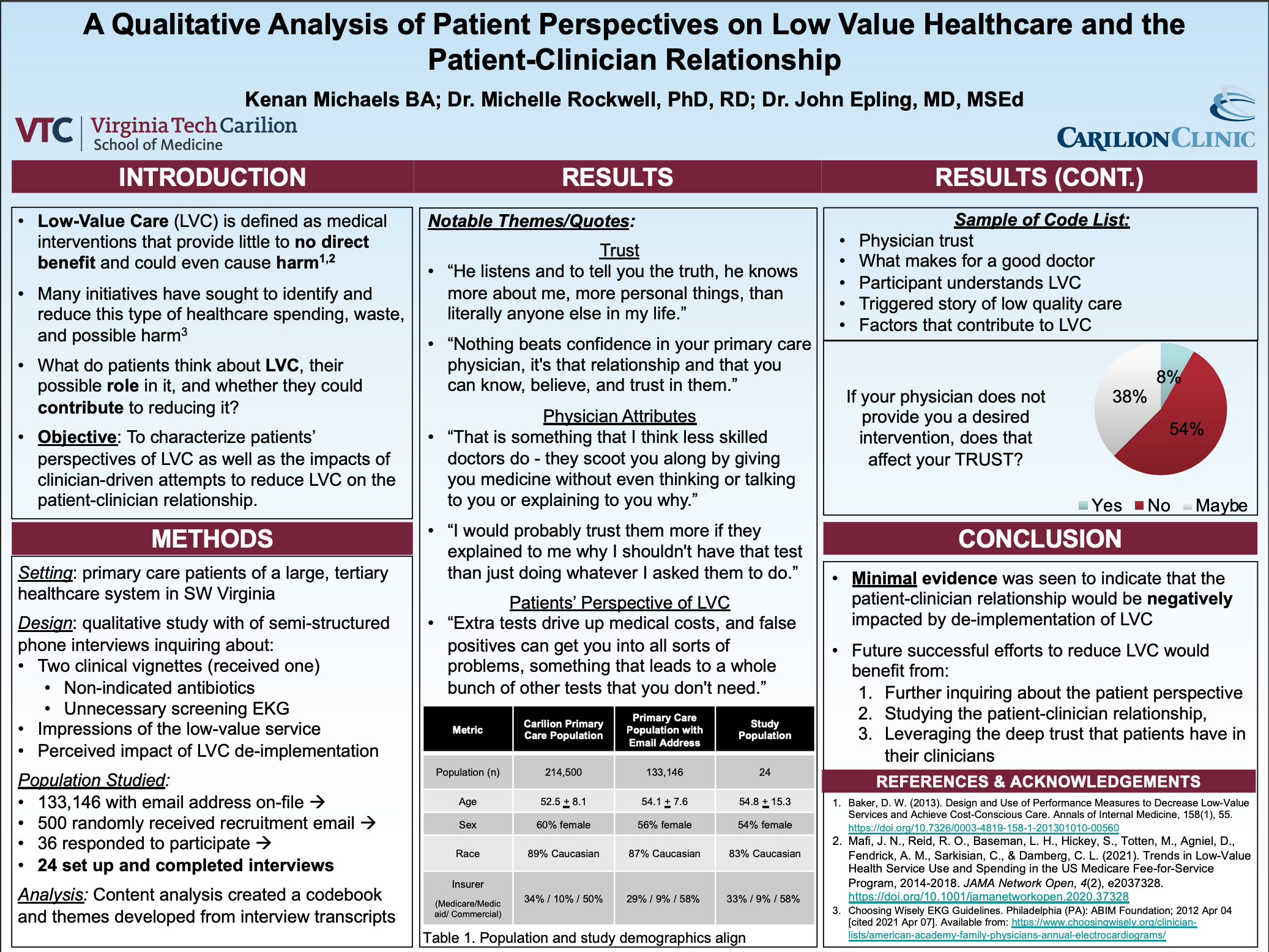
Context: Low value healthcare (LVC) is defined as medical interventions that provide no direct benefit to patients. Many initiatives have sought to identify and reduce this type of healthcare spending, waste, and possible harm; however, little research has focused on patients’ perspectives and the impact of de-implementation on the patient-clinician relationship. Objective: To characterize patients’ understanding of LVC as well as the impacts of clinician-driven attempts to reduce LVC on the patient-clinician relationship. Study Design: A qualitative study consisting of semi-structured phone interviews including a vignette that described a clinician’s decision not to provide LVC services such as antibiotics for acute sinusitis or a LVC screening EKG. Interview prompts also included impressions of the low value service and the perceived impact of LVC de-implementation. Content analysis was performed iteratively to develop a codebook and themes from the interview transcripts. Setting: Primary care patients of a large, tertiary healthcare system (1 million patients, 45 primary care centers) in SW Virginia who were recruited by random email sampling (n=500). Population studied: Participant (n=24) demographics mirror the local primary care patient population: 54.8 years of age, 54% female, 83% White, 33% Medicare/8% Medicaid/58% Commercial. Outcome measures: Overarching themes. Results: Participants had a broad range of understanding of LVC. All participants agreed that they would not want an unnecessary antibiotic prescription yet some felt that they would want to receive a screening EKG. Many also equated LVC with low quality care and were motived to share corresponding stories about a prior negative experience. Despite this, the majority of patients indicated that they place great trust in their clinicians and rely heavily on their direction, likely assisted by the presence of strong communication, trust, and a genuine demeanor. Indeed, more than half of patients stated that the denial of a desired service by their clinician would not negatively affect their relationship. Conclusions: Minimal evidence was seen to indicate that the patient-clinician relationship would be negatively impacted by de-implementation of LVC. Future successful efforts to reduce LVC would benefit from further inquiring about the patient perspective, studying the patient-clinician relationship, and leveraging the deep trust that patients have in their clinicians.
Dennis Baumgardner, MD
11/19/2021Very well done study, poster and oral presentation. Thank you! Dennis