SRFP041: Exploring barriers to LARC placement training for family medicine residents (Pearls)
Komal Soin, MD, MPH; Liana Kobayashi, DO, MPH; Thomas Quattlebaum, MD; Chien-Wen Tseng, MD, MPH, MS
Abstract
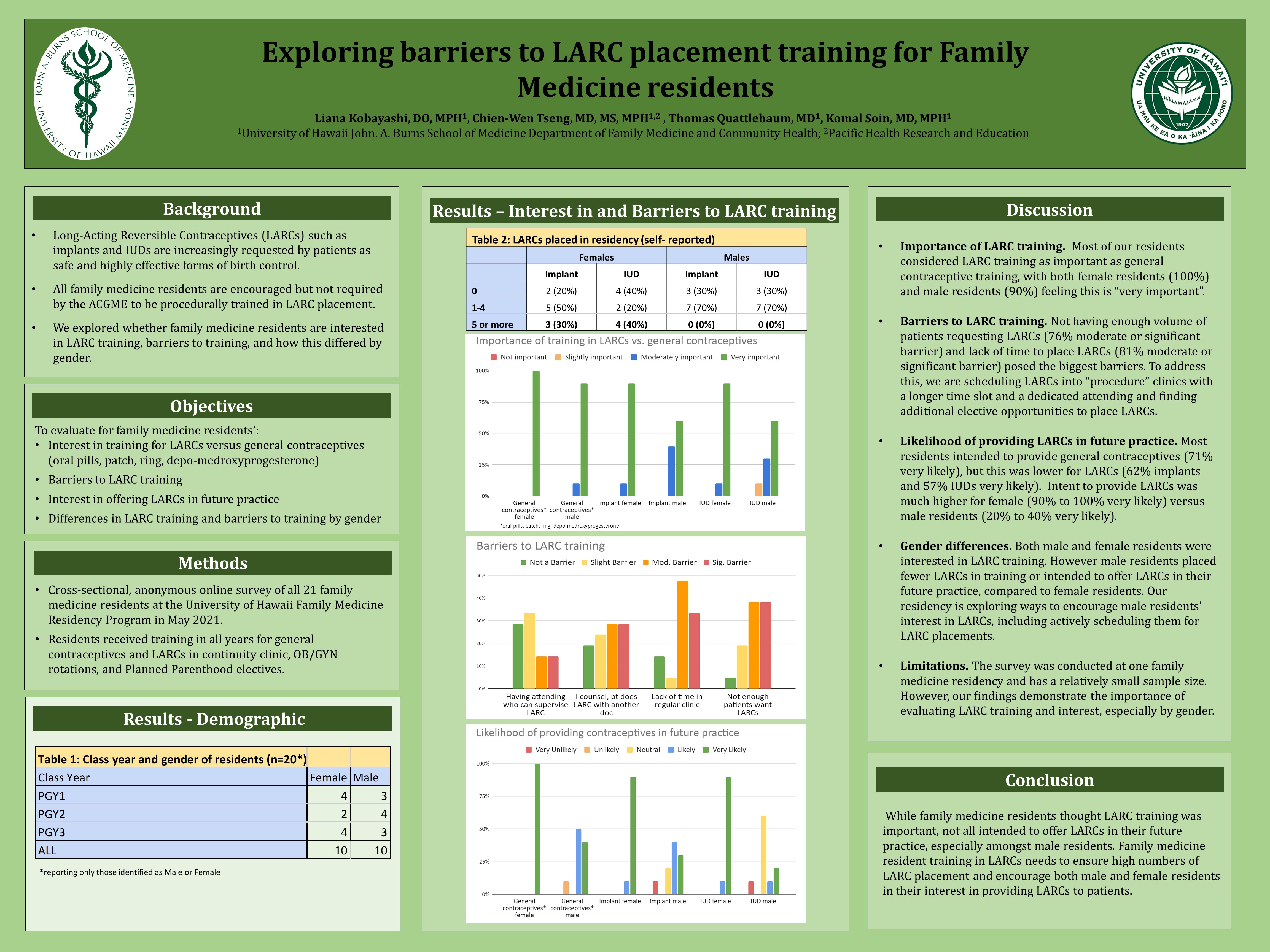
Context: Long-acting reversible contraception (LARC) such as implants and IUDs are highly effective birth control methods. Physicians’ ability to offer LARCs is important for patient access and LARC training is recommended by the ACGME. At the University of Hawaii Family Medicine Residency Program, we explored residents’ interest in LARCs and difficulties experienced with LARC training. Our goal is to design a better curriculum to train family physicians who are competent and confident to insert LARCs in their future practice. Objectives: To evaluate residents’ interest in providing LARCs and barriers to LARC training. Study Design: Residents received general contraceptive and LARC training in their continuity clinics, OB/GYN rotations, and electives at Planned Parenthood. Evaluation of their LARC training experience consisted of a cross-sectional online survey conducted in May 2021. Setting: Community-based family medicine residency program. Population Studied: Family medicine residents. Results: Of the 21 residents (100% response), nearly all considered it “very important” for family medicine training to include general contraceptive counseling (95%) though this was lower for implant (76%) and IUD training (76%). The most common barrier (“moderate” or “significant”) to LARC training was lack of time (81%). Most residents reported 30 minute or less was sufficient for general contraceptive counseling (95%) but not for same-day implant (24%) or same-day IUD placement (14%). Other barriers included too few patients requiring LARCs (76%), doing initial contraceptive counseling but follow-up LARC placement done by different clinician (58%), and attending not available (38%). Regarding intentions after training, female versus male residents reported much higher rates of being “very likely” to provide general contraceptive counseling (100% vs 40%), implant (90% vs 30%) and IUDs (90% vs 20%) in their future practice. Conclusions: Most residents considered LARC training to be very important for family physicians but interest in providing LARCs in future practice was significantly higher amongst female versus male residents. Major barriers which need to be addressed with LARC training are that LARC placement takes time (scheduling into a procedure clinic may help), needs required volume (may need specific electives with opportunity to place LARCs), and gender differences with regards to interest in contraceptive counseling after training.
Jack Westfall
jwestfall@aafp.org 11/21/2021Thanks for your terrific work on this research. Hope we can connect.