SRFP007: Affording Telemedicine Medication Abortion: Examining A Sliding-Scale Payment Option and Patient’s Ability to Pay
Sajal Sanan; Emily Godfrey, MD, MPH; Rebecca Gomperts, MD, PhD, MPP; Nikeeta Shah, BA, MPH; Anna Fiastro, MPH, MEM
Abstract
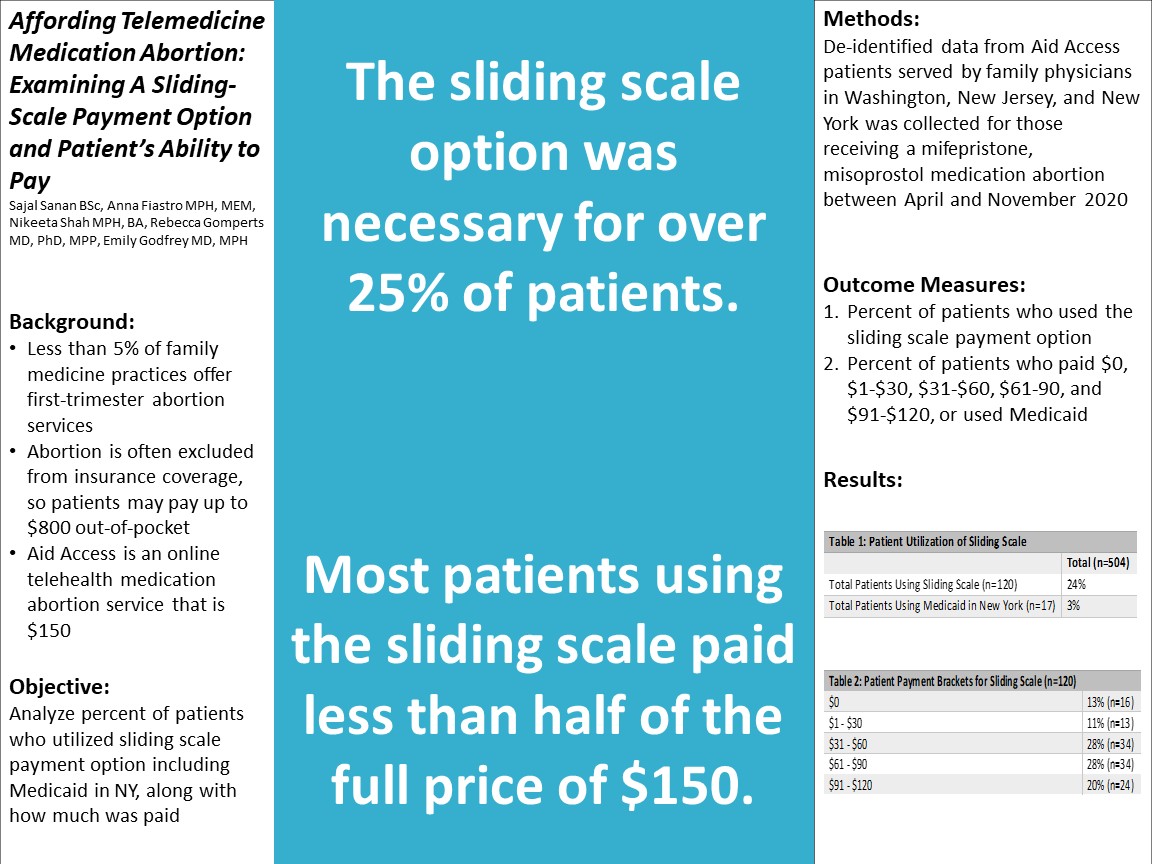
Context: Currently, less than 5% of family medicine practices offer first-trimester abortion services, which means that most patients must seek services at specialty family planning facilities. Since abortion is often excluded from insurance coverage, patients pay up to $800 out-of-pocket. Medication abortion via telehealth is much cheaper ($150-$400). Still, many patients cannot afford this amount. To expand affordability, Aid Access – an asynchronous clinician-supported online abortion service - implemented a sliding-scale payment option that allows patients who ask for a discounted rate to choose a payment amount between $0 and $150 or use Medicaid if located in New York (NY). With the availability of telemedicine, more family medicine providers are starting to offer medication abortion services. It is important to understand the financial needs of patients seeking abortion so family physicians can implement payment options that increase access to these essential services. Objective: Analyze percent of patients who utilized sliding scale payment option including Medicaid in NY, along with how much was paid. Study Design: Retrospective chart review. Setting or Dataset: De-identified data from Aid Access patients served by family physicians in Washington (WA), New Jersey (NJ), and NY, including payment information. Population Studied: Patients who received mifepristone, misoprostol medication abortion through Aid Access in WA, NJ, and NY between April and November 2020 (n=504). Main and Secondary Outcome Measures: (1) Percent of patients who used the sliding scale payment option; (2) Percent of patients who paid $0, $1-$30, $31-$60, $61-90, and $91-$120, or used Medicaid. Results: Out of 504 patients, 24% (n=120) paid for their medication abortion use the sliding scale option and 3% (n=17) used Medicaid. Of the 120 patients using the sliding scale: 13% (n=16) paid $0, 11% (n=13) paid $1-$30, 28% (n=34) paid $31-$60, 28% (n=34) paid $61-$90, and 20% (n=24) paid $91-$120. Conclusions: Although most patients paid full price ($150) for their abortion, the sliding scale option including Medicaid was necessary for over 25% of patients. Of those who utilized the sliding scale, most patients paid less than half of the full price. In order to provide medication abortion services to those who need it, it is important to implement payment options such as the sliding-scale method.
Debra Stulberg
stulberg@uchicago.edu 11/20/2021Great poster! Thank you for this work. In future analyses, I'd love to see more about the option to use Medicaid in states where abortion is covered. With more emerging telemedicine abortion providers, I think it's important to assess whether patients whose insurance plans (including Medicaid) cover abortion actually know this and have the option to use their insurance. And of course, many plans still don't cover it, and we should measure the impact of that as well! But in the meantime I am happy to see the use of sliding scale option when people need to pay out of pocket.