PRP044: How residential mobility may influence estimates of association between community-level risk factors and health outcomes
Teresa Schmidt, PhD; Miguel Marino, PhD; Erika Cottrell, PhD, MPP; Sophia Giebultowicz, MA; Andrew Bazemore, MD, MPH; Jené Grandmont
Abstract
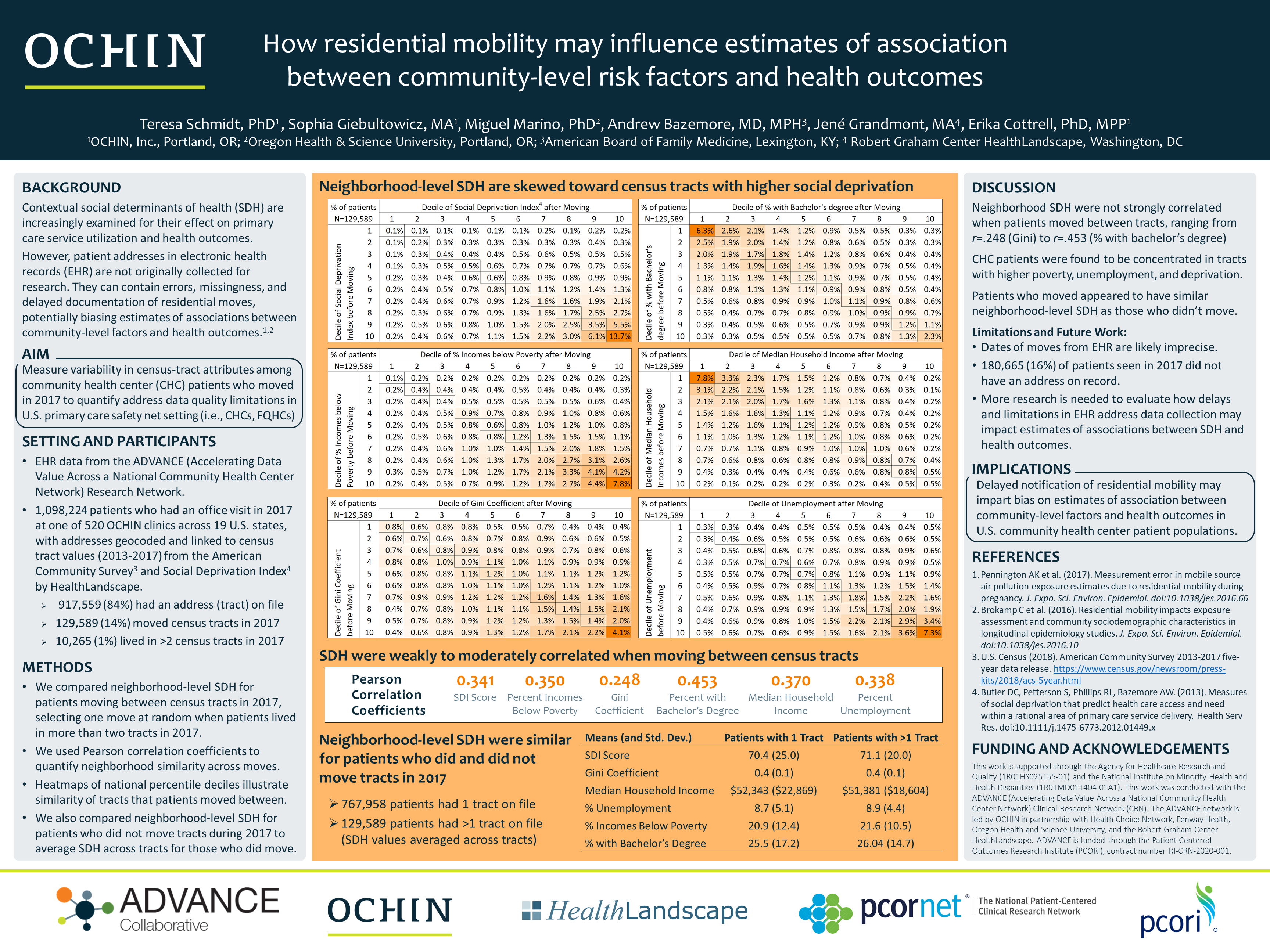
Context: Contextual social determinants of health (SDH) are increasingly examined for their effect on primary care service utilization and health outcomes. However, when sources of patient address history are not originally collected for research, they can contain errors, missingness, and delayed documentation of residential moves. Using the wrong address has been found to meaningfully bias estimates of associations between community-level factors and health outcomes. Objective: To quantify address data quality limitations in a US primary care safety net setting (i.e., community health centers (CHCs) and Federally Qualified Health Centers (FQHCs)), variability was measured in census-tract attributes among a subset of patients who moved in 2017. Study Design: Cohort study of patients visiting any of 520 OCHIN safety net clinics in 19 US states during calendar year 2017. Setting or Dataset: Electronic health record (EHR) data from OCHIN’s EHR system, including historical address records geocoded to 2010 Census tracts by HealthLandscape and linked to American Community Survey indicators and the Social Deprivation Index (SDI). Population studied: Among the 1.1 million patients visiting OCHIN safety net clinics in 2017, 128,950 (11.7%) had traceable evidence of a move between census tracts that same year. Outcome Measures: Percentiles were calculated on tract-level attributes, including percentages of unemployment, poverty, undergraduate degrees, median household income, and the SDI, to evaluate the proportion of patients who moved between tracts with similar versus different attributes. Correlations were calculated between old and new census tract attributes to quantify the degree of similarity across moves. Results: Patients are expected to move between census tracts with similar attributes (e.g., within the same national percentage decile) more often than between tracts with different attributes. A table for each tract-level variable will illustrate the percentage of patients moving to and from each decile in matrix form, with patients who moved between similar tracts captured along the diagonal. Correlations will provide an estimate of error in tract-level attributes if using the wrong address to measure associations between SDH and primary health care utilization or health outcomes. These estimates and distributions will inform future research on SDH about the extent of potential bias when relying on imperfect address history data.
Diane Harper
harperdi@med.umich.edu 11/21/2021This is very interesting. I would ask you to think about how disruptive it is. We know BRFSS continues year after year and some measures do correlate with claims or medical record data, but many do not. And this lack of accuracy does not stop people from the BRFSS analyses. If you can prove that we don't have to watch where the addresses go, then that will simplify future research : ) . Thank you for sharing with us at NAPCRG.