PRP051: Implementing a Care Planning Study: A Patient-Oriented Approach
Paulette Lail Kashiri, MPH; Alex Krist, MD, MPH; Jennifer Hinesley, PsyD; Benjamin Webel, BA; Amy Huebschmann, MD, MS; Hannah Shadowen, MPH; Kristen O'Loughlin, MA, MS; Marshall Brooks, PhD
Abstract
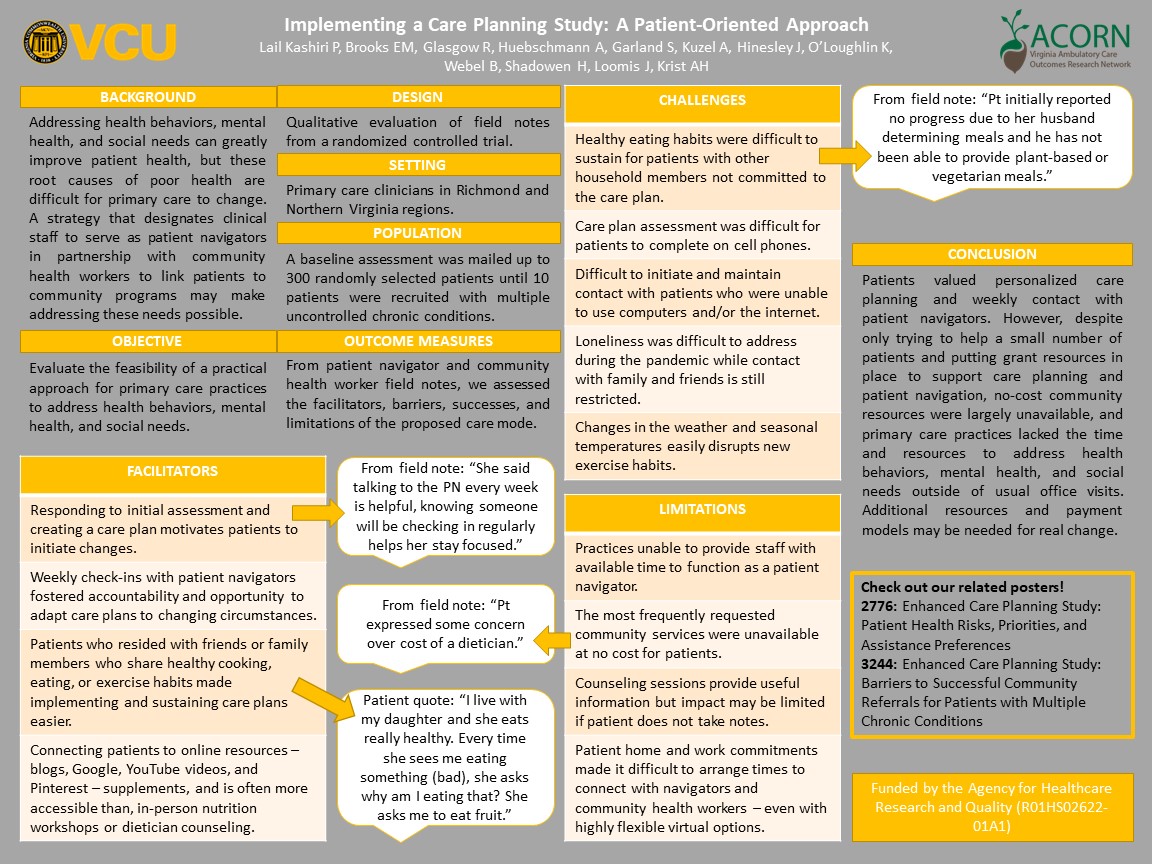
Context: Addressing health behaviors, mental health, and social needs can greatly improve patient health, but these root causes of poor health are difficult for primary care to change. A strategy that designates clinical staff to serve as patient navigators in partnership with community health workers to link patients to community programs may make addressing these needs possible. Objective: Evaluate the feasibility of a practical approach for primary care practices to address health behaviors, mental health, and social needs. Study Design: Qualitative evaluation of field notes from a randomized controlled trial. Setting: Primary care clinicians in the Richmond Metropolitan and Northern Virginia regions. Population: A baseline assessment was mailed to up to 300 randomly selected patients per clinician with cardiovascular disease or risks, diabetes, obesity, or depression, until 10 patients per clinician with uncontrolled multiple chronic conditions were recruited for participation. Intervention: Participants complete a baseline health risk assessment via My Own Health Report (MOHR). Patients select one or two risks to develop a personalized care plan. A patient navigator checks in with the patient weekly to assess the patient’s progress, answer questions, and provide any additional resources, including connecting the patient to a community health worker and community programs. Outcome Measures: From the patient navigator and community health worker field notes documenting support provided and patient experience, we assessed the facilitators, barriers, successes, and limitations of the proposed care mode. Results: Preliminary findings demonstrated four common themes: 1) patients value weekly check in’s and think this helps them accomplish their goals, 2) no clinicians had staff with available time to function as a patient navigator, 3) the most frequently requested community services were not available at no cost for patients, and 4) patient home and work commitments made it difficult to arrange times to connect with navigators and community health workers – even with highly flexible virtual options. Conclusions: Despite only trying to help a small number of patients and putting grant resources in place to support care, primary care practices and communities lacked the time and resources to address health behaviors, mental health, and social needs outside of usual office visits. Additional resources and payment models may be needed for real change.
Bill Kerns
11/21/2021Great work, Paulette, thank you! We are looking at how to best do care managers for our practice, so this information is timely and useful. For example, we need to ask the hospital and community SW's and CM's what they have versus what they need, etc.