PCR080: Utilization of 15 Low Value Services within Primary Care of a Southwest Virginia Health System in 2019
Michelle Rockwell, PhD, RD; John Epling, MD, MSEd; Kenan Michaels, BA; Kyle Russell; Beth Bortz, MPP
Abstract
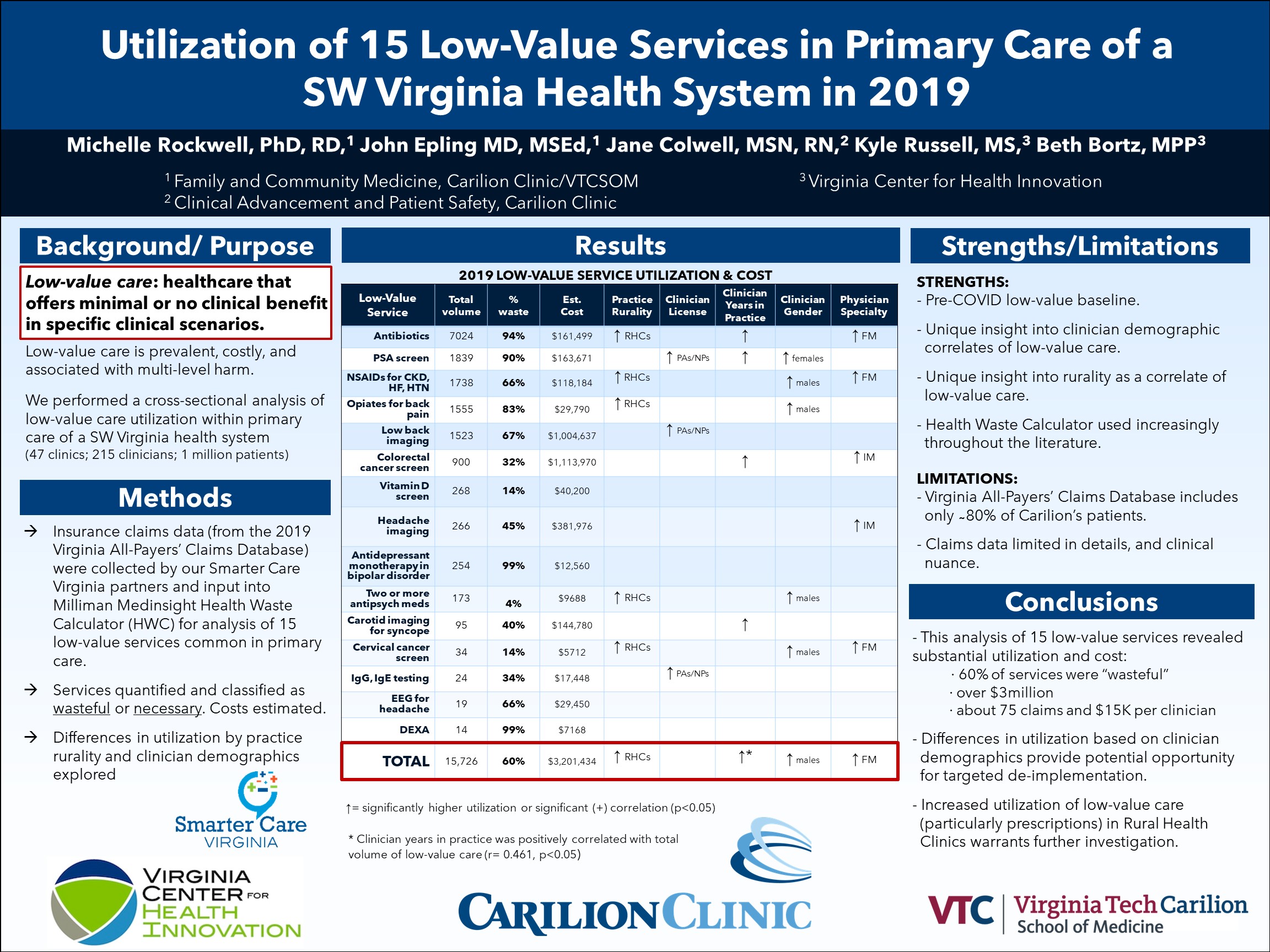
Context: Low-value care (LVC) describes healthcare services that offer minimal or no clinical benefit and may be associated with patient harm, unnecessary costs, and wasted use of resources. Objective: To explore utilization of LVC within a SW Virginia health system (47 clinics, approx. 1 million patients) and to identify factors associated with LVC utilization over the course of one year. Study Design: Cross-sectional analysis of insurance claims using Milliman MedInsight Health Waste Calculator (HWC) for 5 screening tests, 5 diagnostic tests, and 5 prescriptions commonly utilized in primary care. The HWC classifies service utilization as “wasteful” or “necessary” based on USPSTF, Choosing Wisely, and other professional recommendations and guidelines. Setting or Dataset: Virginia All-Payers’ Claims Database claims and internal records (demographics) for 2019. Population studied: Clinicians (n= 211) included physicians, nurse practitioners, and physician’s assistants (n=134, 53, and 24, respectively) serving in primary care for at least 9 months of 2019. Outcomes measures: For each service: total, wasteful, and necessary claims; estimated spend (average dollars paid to health system across all payers); and utilization by clinician demographics. Results: Overall, 15,726 wasteful claims (60% of total claims) for the 15 services were made in 2019, representing an estimated $3,201,434 (averaging 74.5 claims and $15,173 per clinician). Wasteful antibiotics for acute upper respiratory infection (7024 claims), PSA screening (1839 claims), and NSAIDs for patients with CKD, heart failure, or hypertension (1738 claims) were the highest utilized individual services. Although utilized at a lower rate, wasteful colorectal cancer screening ($1,113,970), low back pain imaging ($1,004,637), and imaging for uncomplicated headache ($381,976) were the costliest services utilized. Total wasteful utilization rate was associated with clinicians’ years in practice (r= 0.461, p<0.05), higher in male clinicians, and higher in family medicine physicians (compared with general internists) (p<0.05). Estimated wasteful spend per clinician was higher among general internists (p<0.05). Conclusions: The substantial LVC utilization and expense observed, along with noted variability in utilization based on clinician demographics, will inform interventions to reduce LVC within this health system.
Jack Westfall
jwestfall@aafp.org 11/20/2021Thanks for your terrific work on this research. Hope we can connect.