PRP094: Tribally Engaged Approaches to Lung Screening (TEALS) Study – Year 2 Pilot
Zsolt Nagykaldi, PhD; Kathleen Dwyer, PhD, RN; Mark Doescher, MD, MSPH; Dorothy Rhoades, MD, MPH; Brook McCann, RN; Cara Vaught, MPH
Abstract
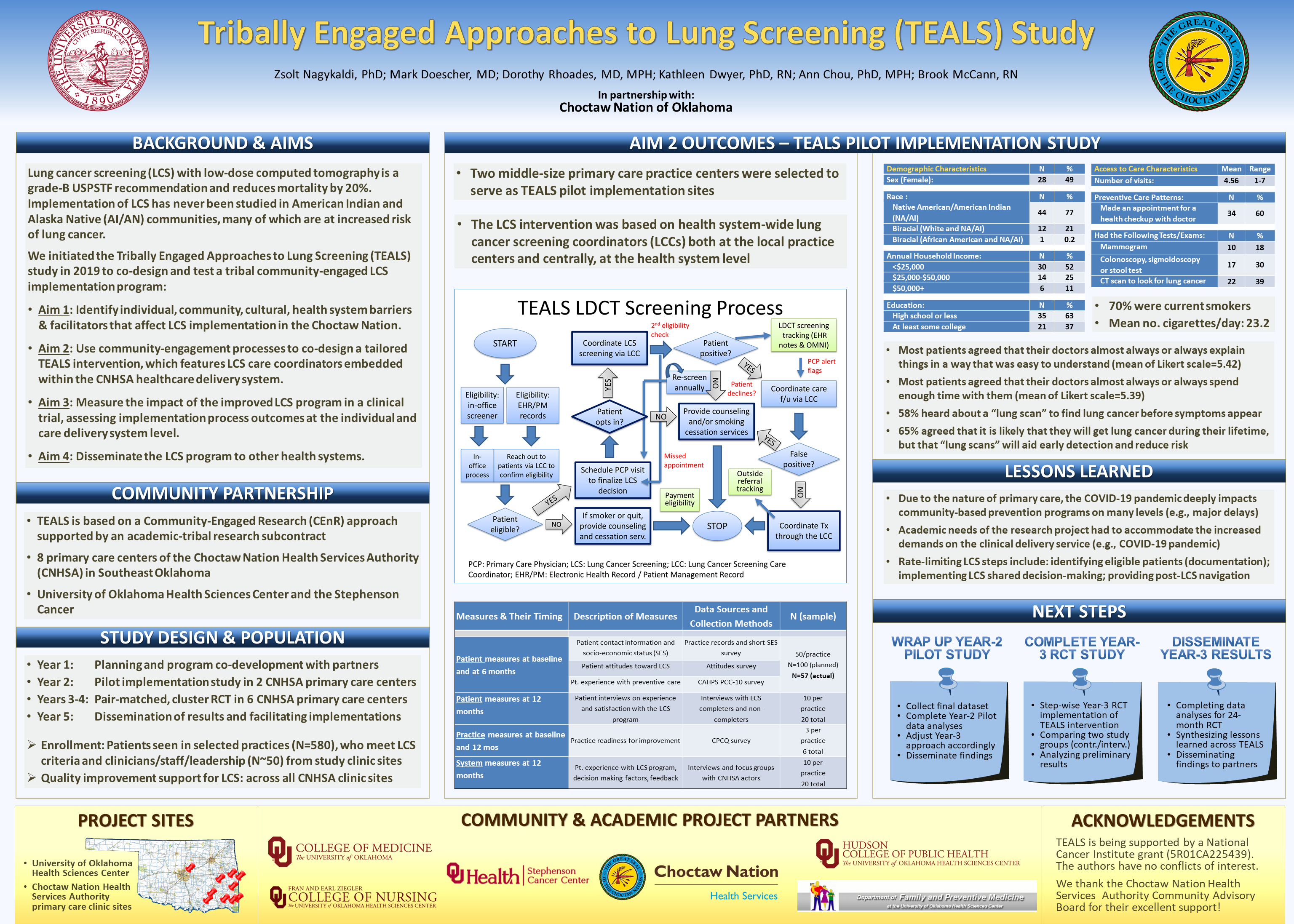
Context: Lung cancer is the leading cause of cancer mortality among American Indians and Alaska Natives (AI/AN), and AI/AN have worse lung cancer incidence rates, survival, and death compared to the general population. Although lung cancer screening (LCS) with low-dose computed tomography is a grade-B USPSTF recommendation, uptake of LCS has been slow in most healthcare systems. LCS implementation among AI/AN has not been studied before in detail.
Objective: To address this knowledge and implementation gap, we initiated a multi-phase, 5-year “Tribally Engaged Approaches to Lung Screening" (TEALS) study in 2019 to co-design and test a tribal community-engaged LCS implementation program.
Setting: TEALS will be conducted in 8 primary care centers of the Choctaw Nation Health Services Authority (CNHSA) in Southeast Oklahoma using a Community-Engaged Research (CEnR) approach.
Study Design: In Year 2 of TEALS, we initiated a pre-post pilot implementation study in 2 CNHSA health centers to prepare for a subsequent RCT.
Population Studied: AI patients (N=100), who meet LCS criteria and clinicians/staff/leadership (N~20) from all CNHSA primary care centers.
Intervention: Two CNHSA practices received EHR reminders for LCS and access to smoking cessation services, in addition to care system improvements, including an LCS Care Coordinator, quality benchmarking and feedback, academic detailing, practice facilitation, and technical support.
Outcomes: Changes in LCS care pathways and care delivery (primary), patient morbidity profile and care experiences (secondary/patient-level), and practice LCS care system improvements (secondary/practice-level).
Results: By the end of Year 2, our team will have implemented and evaluated a pilot LCS program in 2 CNHSA health centers. Many lessons will have been learned regarding major barriers and some solutions arising from the implementation and from the COVID-19 pandemic.
Future Steps: Initiation of a CHNSA-wide RCT in Years 3 & 4.
Objective: To address this knowledge and implementation gap, we initiated a multi-phase, 5-year “Tribally Engaged Approaches to Lung Screening" (TEALS) study in 2019 to co-design and test a tribal community-engaged LCS implementation program.
Setting: TEALS will be conducted in 8 primary care centers of the Choctaw Nation Health Services Authority (CNHSA) in Southeast Oklahoma using a Community-Engaged Research (CEnR) approach.
Study Design: In Year 2 of TEALS, we initiated a pre-post pilot implementation study in 2 CNHSA health centers to prepare for a subsequent RCT.
Population Studied: AI patients (N=100), who meet LCS criteria and clinicians/staff/leadership (N~20) from all CNHSA primary care centers.
Intervention: Two CNHSA practices received EHR reminders for LCS and access to smoking cessation services, in addition to care system improvements, including an LCS Care Coordinator, quality benchmarking and feedback, academic detailing, practice facilitation, and technical support.
Outcomes: Changes in LCS care pathways and care delivery (primary), patient morbidity profile and care experiences (secondary/patient-level), and practice LCS care system improvements (secondary/practice-level).
Results: By the end of Year 2, our team will have implemented and evaluated a pilot LCS program in 2 CNHSA health centers. Many lessons will have been learned regarding major barriers and some solutions arising from the implementation and from the COVID-19 pandemic.
Future Steps: Initiation of a CHNSA-wide RCT in Years 3 & 4.
Diane Harper
harperdi@med.umich.edu 11/21/2021This is wonderful research! You state that it is community engaged research project. Were you funded by NCI before you engaged with the community? How did the community define your grant submission? I would like to connect about future opportunities. Thank you for sharing your work with NAPCRG.