PCR023: Diagnostic accuracy of a new COVID-19 antigen test obtained by mid-turbinate swab
John Epling, MD, MSEd; Matt Lowery, MHS, RN; Alexandra Mahoney; Anthony Baffoe-Bonnie, MD; Tonja Locklear, PhD; Martha Tenzer, BA; Paul Skolnik
Abstract
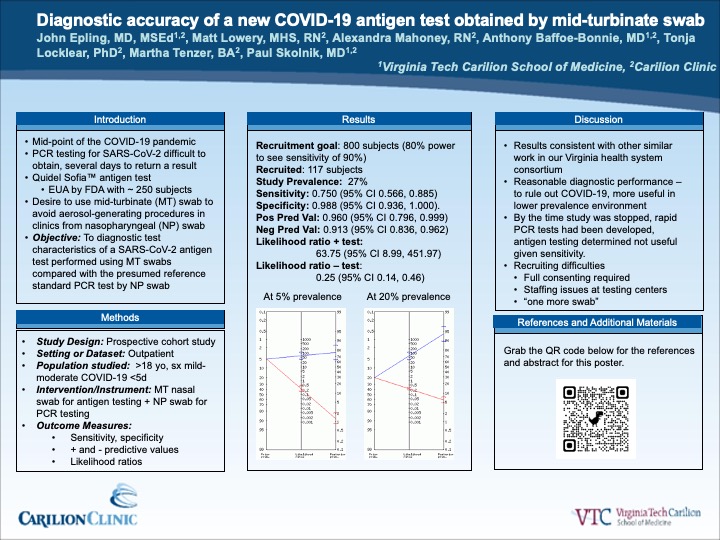
Context: At the mid-point of the COVID-19 pandemic, polymerase chain reaction (PCR) testing for SARS-CoV-2 was difficult to obtain and took several days to return a result. Our health system wished to explore the use of the Quidel Sofia™ antigen test to diagnose COVID-19 in our primary care clinics, but the test was approved for emergency use authorization by the US Food and Drug Administration with only 250 test subjects. In addition, because it was important to avoid aerosol generating procedures in primary care clinics, it was necessary to test the diagnostic performance of the antigen test using mid-turbinate (MT) swabs rather than the approved nasopharyngeal (NP) swab technique. Objective: To assess the diagnostic test characteristics of a SARS-CoV-2 antigen test performed using mid-turbinate nasal swabs compared with the presumed reference standard PCR test by NP swab. Study Design: Prospective cohort study. Setting or Dataset: Outpatient. Population studied: Adults with symptoms consistent with mild-moderate COVID-19. We attempted to recruit 800 subjects to provide statistical assurance that the test sensitivity was at least 90%. Intervention/Instrument: After informed consent, subjects underwent MT nasal swab for antigen testing followed by NP swabbing for PCR testing. Outcome Measures: Sensitivity, specificity, positive and negative predictive values, and likelihood ratios, all with associated 95% confidence intervals. Results: Due to recruitment difficulty (subject reluctance and staffing issues at the testing centers), we recruited only 117 subjects. Sensitivity was 0.750 (95% CI 0.566, 0.885), and specificity was 0.988 (95% CI 0.936, 1.000). Positive Predictive Value was 0.960 (95% CI 0.796, 0.999) and Negative Predictive Value was 0.913 (95% CI 0.836, 0.962). The likelihood ratio for a positive test was 63.75 (95% CI 8.99, 451.97) and the likelihood ratio for a negative test was 0.25 (95% CI 0.14, 0.46). Conclusions: This antigen test for SARS-CoV-2 was of reasonable clinical utility in a low prevalence environment but concerns about the actual prevalence of COVID-19 and the ramifications of false negatives limited its use. Difficulty recruiting subjects and the resultant delay in the results made it impossible to implement this antigen testing in primary care practices, but it is hoped that these data will contribute to the accumulation of evidence about diagnostic testing for COVID-19.
Jack Westfall
jwestfall@aafp.org 11/19/2021Terrific poster and presentation. Thanks for your work showing the role of primary care in the nitty-gritty of COVID-19 response and recovery. Thanks